ED Frequently Asked Questions
The Emergency Department (ED) is a dedicated area in a hospital where trained teams of nurses, doctors and allied health professionals work in a coordinated way to assess, stabilise and decide the best “next step” in the management of all patients. This involves the prioritised evaluation and treatment of patients with time-critical healthcare needs, including their initial emergency interventions and their referral to inpatient services; certain outpatient services (e.g. fracture clinics) or their discharge home for follow up by their General Practitioner (GP).
Because of the high public profile of any ED as the ‘shop window’ of a hospital, there is much written and spoken about how well or otherwise EDs appear to function. As this commentary is frequently ill-informed and confuses wider healthcare system issues with ED issues this series of FAQs is intended to explain how EDs work and explain some of the context in which they operate.

What happens when I visit the Emergency Department (ED)?

Background Information
A visit to the ED can be a stressful event for patients and families. The following information will help you to understand the process and will help you know what to expect at each step along the journey.
Patients arrive to the ED in a number of ways. You may be referred by your GP or primary healthcare provider, brought by ambulance or you may arrive yourself.
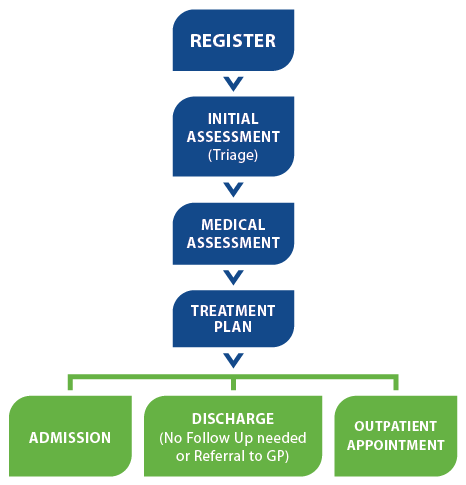
Arrival to the ED
On arrival to the ED, a member of the administrative staff will obtain general registration information about you (name, date of birth, contact details in case of an emergency).
 A statutory government fee is charged to each patient that attends the Emergency Department.
A statutory government fee is charged to each patient that attends the Emergency Department.
Following this, an experienced nurse will assess you. This assessment is called triage and is designed to ensure that seriously ill patients are seen first.
Patients are then assigned a triage category as follows:
- Triage 1: Immediate Resuscitation
- Triage 2: Emergency
- Triage 3: Urgent
- Triage 4: Semi-urgent
You will then be seen by a healthcare worker in order of urgency rather than your arrival times. This is to ensure that the patients with more severe symptoms or injuries are treated before those with less serious conditions.
Please be aware that:
- As an entry point to the hospital, a lot of activity occurs behind the ED waiting room doors. The number of people in the waiting room is often not an indication of how busy the ED team is. If your symptoms worsen, following triage, please inform the Triage nurse immediately.
- Some tests and treatments may need to be arranged. Once the test results are available and the treatments are completed, these will be reviewed with you by your healthcare worker. At this point, a plan will be made for follow-up care or admission to the hospital.
- Sometimes, your nurse/ doctor may get interrupted to respond to another emergency. They will return as soon as that emergency is under control.
Following your medical assessment
Following your medical assessment and treatment patients maybe admitted to the hospital, transferred to another hospital or discharged home with the appropriate follow up care (GP, specialist team or outpatient department).
If your particular case requires admission to a hospital, further evaluation by a team member of the admitting consultant may be required, while you are in the Emergency Department.
When a decision to admit occurs, your bed is arranged on the appropriate ward. As this type of admission is not pre-arranged, it may take time for a bed to become available on a ward. During this time, your care will be provided by the Emergency Department staff.
While every effort is made to streamline this process, you may encounter significant delays at each step along your journey.
What is Emergency Medicine?
Emergency Medicine is the medical specialty recognised by the Medical Council as providing immediate and urgent treatment for patients with the full spectrum of acute illness, injury and behavioural problems.
Information: This unscheduled care is provided 24 hours a day, 7 days a week, 365 days a year.
A Consultant in Emergency Medicine is trained in the assessment, resuscitation and initial treatment of emergency illness and injury of all types. Most of his/her work is based in the Emergency Department, although he/she may be involved in other parts of the delivery of emergency care e.g. providing advice or direct assistance to paramedics or GPs before the patients arrive in the ED, training of staff in other specialties etc.
EDs are staffed by teams of healthcare workers, including doctors, nurses, administrative staff and porters. Some EDs have dedicated social workers, physiotherapists, occupational therapists and radiographers. Staff in particular EDs may provide other services including mental health assessment; social work assessment; bereavement care; in-patient ward care (sometimes called Emergency Observation Medicine, Chest Pain Assessment or Clinical Decision Units); pre-hospital support at the scene of incidents; tele-medical advice for maritime emergencies; injury prevention; health promotion activities and Major Incident response.
Emergency Medicine teams call upon and coordinate support from other hospital specialties and services to meet the care needs of the patients they serve. Emergency Medicine has close connections with many other services within local communities; including the ambulance, fire and police services, GPs, first aid training, social services and other community services.
Why are some patients seen sooner than others
Logical Order of Cinical Need
Patients attending EDs are attended to in a logical order which is based on a patient’s clinical need and not simply their order of arrival. Patients with serious illness or injury or a condition that has the potential to rapidly become more serious will be seen before those with less serious conditions. This prioritisation of patients based on clinical need is called Triage and a standard Triage System is used nationwide to ensure safety and fairness. The process is similar to that used in other countries.
Triage systems use the patient’s symptoms and a focussed examination by a nurse or doctor. More seriously ill and injured patients who need to be seen immediately may arrive in the ED at any time. Patients who experience a change in their condition after having been triaged should always report the change to the triage nurse (or reception staff if the nurse is busy with another patient).
Why are Emergency Departments often crowded?
 Many factors contribute to crowding in Irish EDs. In most hospitals the leading cause is the delay in admission to a hospital bed of patients who have had their initial emergency care given in the ED but who need on-going hospital care or cannot safely be discharged. The presence in an ED of admitted hospital inpatients waiting on trolleys (inpatient boarders) results in a loss of clinical spaces in which to see new ED patients causing delays and further crowding. Many Irish EDs are too small to appropriately accommodate the numbers of patients who need emergency treatment. Compared to international standards, many Irish EDs are deficient from an infrastructure point of view and need to be rebuilt or extended to reach an acceptable standard of accommodation. Just as it is difficult for EDs to work effectively if they are crowded, it is also difficult for them to work efficiently if they are too small or poorly designed.
Many factors contribute to crowding in Irish EDs. In most hospitals the leading cause is the delay in admission to a hospital bed of patients who have had their initial emergency care given in the ED but who need on-going hospital care or cannot safely be discharged. The presence in an ED of admitted hospital inpatients waiting on trolleys (inpatient boarders) results in a loss of clinical spaces in which to see new ED patients causing delays and further crowding. Many Irish EDs are too small to appropriately accommodate the numbers of patients who need emergency treatment. Compared to international standards, many Irish EDs are deficient from an infrastructure point of view and need to be rebuilt or extended to reach an acceptable standard of accommodation. Just as it is difficult for EDs to work effectively if they are crowded, it is also difficult for them to work efficiently if they are too small or poorly designed.
It needs to be understood that the ED has no control over the access to inpatient beds. The delay in admission to a bed is largely due to there being inadequate numbers of acute hospital beds (the type of bed ED patients need) or that these beds are taken up with patients whose acute care is finished and who would be better cared for in the community but can’t be discharged because of the lack of the necessary supports or funding (delayed discharges).
Patients needing an Intensive Care Unit bed may suffer delays as there is a national shortage of critical care beds.
Why do Emergency Department visits take varying periods of time?
How long will I spend in ED?
 The length of time a patient will spend in an ED is variable and depends on the severity and complexity of their underlying medical problem and the resources available in the ED to see them. All EDs try to deal with anyone who attends an ED as quickly as possible but without compromising on patient safety. The Irish Association for Emergency Medicine firmly believes that all Irish EDs should be enabled to be able to admit or discharge each patient who attends within 6 hours of arrival. While this standard has been accepted in principle by the Health Service Executive (HSE), it has yet to be consistently achieved.
The length of time a patient will spend in an ED is variable and depends on the severity and complexity of their underlying medical problem and the resources available in the ED to see them. All EDs try to deal with anyone who attends an ED as quickly as possible but without compromising on patient safety. The Irish Association for Emergency Medicine firmly believes that all Irish EDs should be enabled to be able to admit or discharge each patient who attends within 6 hours of arrival. While this standard has been accepted in principle by the Health Service Executive (HSE), it has yet to be consistently achieved.
A patient may be in the ED for some hours, particularly if they have a complicated health problem that requires special blood tests, diagnostic imaging (x-rays, scans etc.) or other specialists to help in their medical assessment. It may take the ED team several hours stabilise particularly ill patients.
The nature of emergency care means that the vast majority of ED patients arrive unannounced. Services that do not operate by appointment, especially those such as EDs that provide services that can vary in length from minutes to hours for different patients will always have episodic delays, no matter how well organised they are. Unfortunately, many EDs do not have the necessary resources to provide timely care for all patients, particularly during the busiest times. This may relate to problems with ED crowding; inadequate nursing, medical or administrative staff numbers or inadequate support for the ED from within the hospital.
In the Association’s view, improved ED design, staffing and organisation of care would help reduce waiting times for all patients.
Which types of symptoms usually need Emergency Department assessment?
Symptoms that usually need immediate ED assessment
Emergency Medicine doctors understand that it can be very difficult for members of the public to decide when an individual’s symptoms or medical condition are an emergency. If a patient or a family member thinks emergency care is required, they may come immediately to the ED where they will be assessed by trained staff. Symptoms include:
| Difficulty breathing or shortness of breath | Chest or upper abdominal pain or pressure | Severe abdominal pain | ||
| Vomiting blood | Collapse, sudden dizziness, weakness | New confusion or change in mental status | ||
| Sudden changes in vision | Any sudden or severe pain | Uncontrolled bleeding | ||
| Difficulty speaking | Significant injury | |||
| Severe or persistent vomiting or diarrhoea (most vomiting or diarrhoea can be dealt with by self-care or your GP) | ||||
This is not intended to be a complete or exclusive list.
Symptoms: Phone the Ambulance Service on 999 or 112 if you think the medical condition is, or may become, life-threatening.
Children have particular medical problems and may have different symptoms to adults. The younger the child, the more difficult it can be to fully assess them. Children under the age of three years are particularly susceptible to serious infections such as meningitis, pneumonia, urinary infections etc. Children may also be unable to tell an adult how they feel. Always get immediate medical attention if you think a child is having a medical emergency such as a seizure; persistent high temperature with listlessness or vomiting; blueness around the lips/mouth or hands/feet; an irregular pattern of breathing or short periods of not breathing at all.
Should I go to my GP or the Emergency Department?
On-going Healthcare Needs
A General Practitioner (GP) is the best person to be responsible for an individual patient’s on-going healthcare needs; every person living in Ireland should therefore ensure that they are registered with a GP. After discharge from the ED, the doctor may post or occasionally give a letter to a patient to bring to their GP for follow up care.
It is more appropriate to attend the GP in relation to long-term medical problems unless the problem experienced is likely to require emergency hospital treatment. Chest pain, signs of a stroke or other time-critical conditions should result in a patient going immediately to their nearest ED.
With less urgent medical conditions, it is better to discuss symptoms with a GP or Primary Care out-of-hours service before going to the ED. In many of these less urgent situations a GP will be in a position to carry out an examination and provide treatment. In cases of injury a GP may be able to organise to have X-rays and other tests carried out without the need to attend an ED.
A Statutory Charge is levied by the Government for use of the ED service. This charge is currently €100, payable on ED registration. It does not apply if you have a referral letter from a GP and in a number of other circumstances detailed in the relevant statutes.
Some myths about Emergency Departments
There are many myths about Emergency Departments. These range from the types of patients seen there to the appropriateness of certain patients attending to suggestions that there are better alternatives to ED care. This section will explore these issues.
Most patients attending Emergency Departments can be dealt with in Primary Care
There is undoubtedly an overlap between Primary Care (i.e. General Practice) and Emergency Department Care although the extent of this is regularly overstated by commentators. Research evidence from the United Kingdom suggests that approximately 15% of patients seen in EDs there could have been seen and treated in Primary Care. Even allowing for the greater variability in Primary Care provision in Ireland compared to the UK and the difficulties GPs encounter in accessing diagnostics, the figure in Ireland is likely to be broadly similar.
Emergency Departments are full of drunks
There is a public misconception that EDs are ‘full of’ intoxicated patients engaging in antisocial behaviour, a view often trumpeted by uninformed commentators. While intoxicated patients occasionally do cause disruption in EDs, this is generally not the case. People who have taken alcohol or other drugs often require medical assistance, either as a direct result of the substances they have taken or because they are more likely to be injured or develop an acute medical complaint.
EDs provide a 24 hour healthcare service for people, irrespective of the nature of their problem or their social circumstances. Emergency Medicine is the ‘healthcare safety net’ for the community. To do this ED staff adopt a non-judgemental approach to patients who are intoxicated, misuse substances, have social problems or who may be temporarily unable to look after themselves. All EDs should be designed, equipped and staffed to care for patients who are intoxicated or are engaging in anti-social behaviour without this impacting on other service users. All patients have a right to feel safe when they attend an ED and patients and relatives are encouraged to contact staff immediately if they feel uncomfortable or threatened in any way.
There are better options to attending an Emergency Department
The specialty of Emergency Medicine developed internationally, half a century ago, because of the general recognition that individual medical specialties and services (general medicine, general surgery, orthopaedic surgery etc.) were often very good at providing specialty care to patients with a clear diagnosis but were less good at dealing with either critically-ill or -injured patients or those acute but undifferentiated patients who had yet to have a diagnosis made. It was recognised that these groups’ care needs required a specialty whose doctors were trained to resuscitate the very sick and assess and manage the undifferentiated patient before passing them on to the relevant specialty after completion of their initial assessment and treatment.
Not all patients with an acute health care need to be seen in the ED and alternative pathways must exist for these patients. Among the many examples of these include rapid access to outpatient and diagnostic services or end-of-life care for patients with confirmed life-ending conditions but who need hospital care for symptom relief. Patients such as these should not be obliged to attend an ED just to access the service they require.
While the Association sees merit in Acute Medical (or other) Units providing an option for patients with a diagnosed medical condition that need hospital intervention, neither they or other specialty-based assessment units are able to deal with either the undifferentiated patient workload or the sicker group of patients in need of resuscitation where EM doctors and EDs are required. The experience around the world is when alternatives to ED care are provided; the number of patients attending EDs continues to rise, notwithstanding the provision of these new services.
Emergency Departments have unfettered access to the full range of hospital services
Patients (and indeed, other medical practitioners) often assume that Emergency Departments can, or indeed should, facilitate access to the whole gamut of diagnostic and other services provided in a particular hospital or a region. This view results in patients being referred to or attending EDs to seek a specific diagnostic test e.g. an MRI scan or access to a particular service. This is inappropriate and the inability of EDs to facilitate this may cause unnecessary conflict with patients. It needs to be borne in mind that EDs are there to deal with acute emergencies and have no role in the facilitation of other levels of care.
Patients with Minor Illness or Minor Injury contribute to delays for sick patients and add to the ED crowding problem
To the surprise of many, research evidence is clear that patients with minor illness or injury contribute very little to the wait to see a doctor in an ED. At a time when many EDs suffer from crowding as a result of admitted inpatients (inpatient boarders) taking up clinical spaces in an ED, the commonly held, but flawed, view is that if this patient group was seen elsewhere that the crowding problem would be ameliorated. The scientific evidence does not support this view.
In an attempt to optimise access to emergency care for this patient group, many EDs use streaming so that parallel queues are used for different categories of clinical presentation which uses the ED’s clinical resources more efficiently than a single queue.
What should I do if I am disappointed with my experience in an Emergency Department?
EDs welcome constructive comment and use patient feedback to advocate for improved services on an on-going basis. All patients attending an ED are entitled to have their legitimate concerns and complaints addressed by the person in charge of the hospital e.g.the hospital General Manager or Chief Executive Officer.
Contact General Manager or Chief Executive Officer
You should write or phone the hospital’s Complaints Officer (the responsible person’s exact title may vary from hospital to hospital) who will explain how to make your complaint and the process involved. If the problem relates to a clinical care issue he/she will ask the nurse in charge or the responsible Consultant in Emergency Medicine to investigate the complaint and deal with any specific issues you have raised. Depending on the nature of the complaint, the senior doctor or nurse may discuss the matter with you by phone, provide an appointment to discuss the matter with you face-to-face or may respond to you in writing.
It is important to understand that EDs do not have discretion over the payment of the €100 Statutory Charge. This charge is a government levy which is defined in law and applies for use of the ED service by patients who are not exempt from it. It is not in the gift of the ED to quash a bill even if a patient feels that their care didn’t meet their satisfaction.
What are Urgent Care Centres (UCCs)?
Urgent Care Centres may provide care to patients with acute illnesses and injuries that are not thought to be life-threatening. These are often private facilities that aim to maximise convenience and access for some patients with less-serious injuries and illnesses. UCCs cannot provide the level of services available at well-developed EDs and, similarly, are not a substitute for care from a patient’s own General Practitioner.
IAEM has defined a set of minimum requirements for Urgent Care Centres in Ireland. This set of standards is available here.